Transcript
PayPal Holdings, Inc. (PYPL) Q3 2025 Earnings Call Transcript
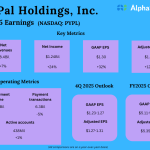
PayPal Holdings, Inc. (NASDAQ: PYPL) Q3 2025 Earnings Call dated Oct. 28, 2025 Corporate Participants: Steven Winoker — Chief Investor…
2 weeks ago
51 min read